

InformationWeek Healthcare IT Priorities Survey of 322 healthcare technology professionals in February 2014 and 363 in January 2013.
Without patient participation, people can, for example, undergo duplicate medical tests when they see different doctors. That could hurt the patient, especially if radiation is involved, and result in extra expenses for payers and for patients responsible for co-payments. But getting patients interacting with their records this way is a big mindset change for doctors and patients.
"Traditionally, when I started practicing way, way back, the healthcare information was really owned by the provider. It was proprietary and part of that was for legal reasons," says Hoffstatter. But the healthcare industry can't ask patients to take a bigger role in their care -- including paying for more of their own treatment -- while also limiting data access. "The problem is we told [patients] for years and years, 'You can't have your information,'" Hoffstatter says. "Now we're saying you should own your information and be [a participant] in patient engagement."
The CIO's role
The CIO is responsible for creating the foundation for a new culture of transparency. Automating routine processes -- such as patching and provisioning of new or expired users -- is critical to giving patients secure access in an environment that frequently changes, Courion's Zannetos says. Usually working in tandem with department heads and healthcare end users, CIOs and their C-level counterparts are charged with implementing systems that encourage consumers to visit and interact with patient portals in order to meet Meaningful Use requirements.

Technology Advice study, August 2014.
Many healthcare providers install patient portals to promote a sense of consumer record ownership or interaction. About half the hospitals in the United States and 40% of physicians had a patient portal, according to Frost & Sullivan's September 2013 study, "U.S. Patient Portal Market for Hospitals and Physicians". Most portals were part of clinicians' practice management or EHR software purchases, the study found. Practices will spend a forecasted $898.4 million on patient portals by 2017, and yet providers often struggle to get consumers to use them. Under Meaningful Use Stage 2, the federal system of incentives and penalties currently in force, providers must ensure 5% of patients use a portal before they attest for compliance. Yet almost two-thirds of organizations report only 0% to 5% of patients are participating, an August report by Peer60 found.
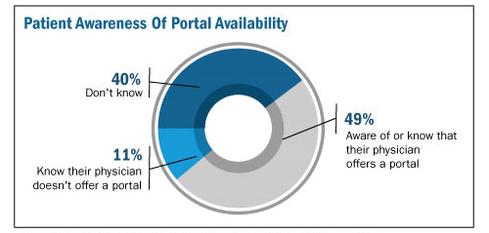
One reason? Patients might not know the portals exist, a recent Technology Advice study on portals revealed. Only 49% of patients knew whether their physician had a portal; 11% knew their doctor did not use a portal; and 40% did not know their physician's portal policy, the study found. Other than billing
or payment notifications, about 48% of primary care doctors did not follow up with patients after a visit and of those who did, only 9% used their portal to do so, Technology Advice found. Instead, they used less cost-effective means, such as phone (24%) or letter (13%).
To encourage portal adoption, CIOs must ensure these systems are easy to use and provide patients with valuable information. Providers typically rely on staff and volunteers to encourage enrollment, often when the patient is admitted to a hospital or during a doctor visit. That's the approach Florida Hospital Celebration Health takes. The hospital is designing a portal where released patients can review their records, watch videos related to their treatment, receive lab information, and stay connected to the hospital.
"We are looking at ways we can leverage technology to keep those patients engaged," says Sandra Reeder, director of nursing at Florida Hospital Celebration Health. "Again, trying to keep them engaged so as soon as they leave so they don't feel everyone's washed their hands of them."
That's also the approach for South Nassau Communities Hospital. The hospital installed FollowMyHealth portals from Allscripts as part of its effort to achieve Meaningful Use Stage 2. Volunteers help patients create accounts while they're at the hospital, and participants receive access to records, lab reports, discharge summaries, and other personal information.
Consumers can populate portal profiles with their photographs, demographic and family history information, and other data, and access their file from any computer, says Rosenhagen. The cloud-based portal is always current, and automatically updates whenever patients are seen as an inpatient at the hospital or emergency room, he adds.
"That's giving the patient more information, at no cost to them, and it's what patients have really been crying for a long time," says Rosenhagen. "The bureaucracy, the way it was set up, never allowed the patient to freely access their information. They always had to pay somebody to get somewhere."
Before EHRs, hospitals in New York could charge up to 75 cents per page in copying fees -- for records that could run to several hundred pages. Downloading patient data to CDs, which South Nassau Communities considered, is time-consuming, inefficient, and costly.
"The only way you can succeed is by being transparent," Rosenhagen says. "The more savvy people get, the more demands will be made and the more a hospital has to respond. They have to be totally transparent and absolutely committed to make it right."
Access can, of course, create the occasional problem if a patient disagrees with a diagnosis. In a case like this, Rosenhagen reviews the EHR entries, brings together the different parties, and determines how clinicians made the diagnosis. When facing an unpleasant nomenclature, some patients fight the entry in their record. Providers must review complaints or disagreements, even if ultimately the doctor's diagnosis is determined to be valid. "If we made a mistake we have to fix it, and we have to find out why it happened and how it happened," says Rosenhagen. "We might also find it's not a mistake" but merely a patient who doesn't want something like alcoholism on his or her medical record.
If the diagnosis stands, South Nassau Communities will include the complaint and the patient's response.
"Every time that record is printed or reviewed by anyone, that complaint in the words of the patient and signed by the patient, dated by the patient, will be available for them as well," Rosenhagen says. "People can make an educated understanding of what took place. It's there, but we may not have found the ability to make that addendum or amendment because we couldn't prove it."
The government mandates healthcare organizations allow consumers to review and annotate their EHRs, although providers don't necessarily have to amend their records if they stand by their original prognosis, says Brenda Tso, associate attorney at healthcare specialists Khouri Law Firm. EHRs can, therefore, include doctors' original diagnoses, patients' disagreements, and the providers' ultimate conclusion. Subsequent providers then can review the entire electronic file, she says.
"I think that was the intent of the laws: To give greater access to the patients but also allow hospitals the ability to make a justified attempt to learn the facts," Rosenhagen agrees. If the facts don't justify changing the record, the hospital needs to be able to make that call and justify the reason why, he says.
Limiting access
As stewards of patient data, it's incumbent on healthcare providers to prevent unauthorized people from accessing records. That includes staff members who might want to nose into a neighbor or ex-spouse's condition, even when they are not treating them. South Nassau installed the patient



